{kind=link}
Five-year longitudinal documentation review
MUSIC JOURNEY
The music journey preserves Bum-Leg Records, recording history, and the path toward ToneLane.
Open Music JourneyToneLane pre-production prototype is now available for testing.
Use Show controls for Help, Pages, Sections, Languages, Search, Play, and Voice. Major destinations open directly; full instructions are in Help.
Open Help for instructions. Open Languages for the language list.
Project Fionigan started from the need to keep a complex medical journey and conference materials organized.
First and foremost, this work is for family, for the medical journey, for finding the right doctor, and for continuing to search for answers.
FND is still a learning journey. Understanding grows over time, and there is still more to learn. Clinicians may not always have the full FND picture either. That is where communication and continuity can break down fast.
This page first started as an online poster and handout. When the conference situation changed, the page became a lived report. That is what the one-page report is supposed to do: keep the important information together when things change.
The public website explains the program. Personal medical records and working continuity reports remain private and patient-controlled.
The rest of this page has the deeper detail.
A plain-language page about FND, communication access, and how Project Fionigan helps keep a patient’s story together when lived explanation becomes difficult.
Project Fionigan keeps fragmented FND information connected, source-linked, and human-readable when lived communication becomes difficult.
New to FND? Functional Neurological Disorder (FND) is a real neurological condition that affects how the brain sends and receives signals, which can cause problems with movement, speech, sensation, thinking, or seizure-like episodes. NIH/NINDS overview.
I am not learning how to have FND. I am learning how to have FND publicly.
FIRST AND FOREMOST
The starting point is a real person living a medical and accessibility journey. Family is in the boat too. Project Fionigan is the navigation layer for that boat: it helps keep the medical journey, documents, questions, access needs, and next steps from scattering.
The website, overlay, pages, documents, and conference materials are context around that journey. The public version stays de-identified and informational.
Current project direction — July 2026
Project Fionigan is now being developed as a data-agnostic continuity framework. Healthcare is its first public implementation, not its only possible use.
The same structure can organize different kinds of source information: identify the source, identify the target, measure the discrepancy, preserve provenance, provide guidance, and leave review and decisions with people.
The newest public direction includes ToneLane as an audio-engineering branch, a question-driven research lane for future FND study, and an automated import review designed to identify missing, duplicated, private, or unresolved material without requiring the user to remember to ask.
Audio connection — prototype
ToneLane is the audio-engineering branch of the same continuity framework. It compares a source recording with a target, identifies measurable differences, offers practical engineering guidance, and leaves the final decision with the human engineer.
The prototype has been built and still needs testing. The intended model is local-first: recordings and project files stay on the user’s machine while the application connects to a current reference database. Future non-identifying statistics may record categories such as the instrument, discrepancy, suggestion tried, number of attempts, and whether the result moved closer to the target.
Imagine if you could make a $20 mic sound like a 58. ToneLane does not promise magic or automatic mixing. It shows the lane, teaches the difference, and lets the engineer use their ears.
Planned early supporter access is $1 per week. The subscription and prototype access are not active yet.
How this became the website
Project Fionigan did not start as a finished website. It started as a conference poster and handout built to explain a one-page clinical continuity report.
The original goal was practical: make a complicated medical story readable fast enough that a doctor, family member, advocate, reviewer, or conference attendee could understand the important facts without digging through scattered records.
Then the conference changed the project. The poster and handout were no longer only static materials. They became a lived report: a way to keep the story, corrections, unanswered questions, source trail, and access needs together while the situation was still moving.
That is why the website looks different from a normal website. It is part public explanation, part accessibility layer, part continuity framework, and part living record of how the project changed in real time.
The website became the story because the problem itself was a continuity problem. The information did not stay connected when it needed to. Project Fionigan keeps the journey, family context, medical questions, accessibility needs, one-page report, poster, and source map from scattering.
Original handout
The original handout pages are shown fully and unedited, like the poster. These were part of the original website/conference material before the website changed during the conference.
FND / emergency bridge
Public FND emergency-department literature describes a known pitfall: FND can arrive in acute care looking like seizure, stroke, movement disorder, or another neurological emergency. The key question in this project is one step more specific.
What happens when the FND / functional movement lane already exists before the emergency?
The de-identified source map shows that the functional-neurology lane, communication-access needs, episode-related speech and hand-use interruption, and source context existed before the later acute-care/legal escalation. The problem was not simply absence of information. The problem was that the information did not follow clearly enough when acute decisions were made.
The legal/custody doorway and the neurological/communication-access doorway can describe the same moment very differently. Project Fionigan is built for that gap: preventing the wrong doorway from becoming the whole story.
Project Fionigan is not anti-medicine and not anti-psychiatry. It is anti-context-collapse.
The goal is to preserve diagnosis, source context, communication method, symptom pattern, open questions, corrections, and next steps so a complex person is not reduced to how they look in one acute moment.
Why it is still a long-scroll page
The long-scroll structure is intentional. It keeps the context together instead of forcing the reader to click through many separate pages while trying to remember where each piece belongs.
The regular page view, floating controls, read-aloud tools, yellow follow mode, search, language buttons, and source map are there to reduce cognitive load. The goal is not a fancy website; the goal is for the important information to stay usable when reading, speaking, typing, memory, stamina, or navigation become difficult.
The source-map cards remain available, but they are secondary to the story. The front door should explain the human path first: medical journey, family in the boat, conference handout, lived report, website, and continuity framework.
School accessibility / EyeGaze branch
The Stafford accessibility material is being added to the Project Fionigan journey as a de-identified source-map branch. It is not being posted as raw school-system records, raw visuals, raw emails, or raw FOIA attachments.
The meaning is preserved: the project now connects medical continuity, school/public accessibility, EyeGaze-style access, school nutrition/menu use cases, and the need for one overlay that can help people move through fragmented systems without hand-dependent navigation.
This is the same rule as the medical side: never remove the line; compress it, de-identify it, source-map it, and keep the raw record private when public posting would expose identities or redaction-risk material.
Public poster
The approved conference poster is part of the public poster/abstract lane.
Project Fionigan was used to organize the poster, handout, website, emails, updates, downloads, and public explanation for this conference.
This is not only an idea being described. It is being used in real time when fine motor control, typing, speaking, or lived explanation become harder to rely on.
First and foremost, this work is for family, for the medical journey, for finding the right doctor, and for continuing to search for answers.
Project Fionigan helps keep the order, documents, corrections, questions, and next steps in one place when typing or speaking gets hard.
Before Project Fionigan carried meaning through structured continuity, similar work was already happening through music. Music can carry timing, emotion, communication, pattern, and participation when ordinary channels are not enough.
Project Fionigan extends that same access idea into FND navigation, medical continuity, and patient communication support.
Project Fionigan helps organize information without removing human control. People provide the source material, computer tools help sort and format it, and a person reviews, corrects, and approves what moves forward.
Computer-assisted processing may include AI tools, but nothing is treated as final until a person reviews and approves it.
This page is built in plain language with an all-inclusive accessibility-first design so it is easier to use when reading, typing, speaking, or fine motor control is difficult.
Use the TL;DR first, then move section by section. The deeper details are below for anyone who wants them. The page supports keyboard navigation, readable spacing, image descriptions, and reduced-motion settings.
FND is still a learning journey. Understanding grows over time, and there is still more to learn every day.
The conference showed that prior presentation experience does not prevent an FND-related communication breakdown. A person may know the setting and still be unable to continue the same way physically.
Clinicians can also miss important parts of the FND picture. When the patient is still learning and the clinician does not have the full FND context either, things can break down quickly.
FND patients may recognize patterns faster than they can organize or explain them out loud. Project Fionigan helps slow the information down into something readable, reviewable, and easier to explain without losing the thread.
This page started as the poster and handout online. As the conference situation changed, it became a lived report of what was happening.
That is the point of the one-page report: when things change, the most important information stays together instead of getting lost.
The page became the place where information could be read back, organized, and kept together when lived explanation was not reliable.
Prior presentation experience matters. This was not unfamiliar territory, stage fright, or confusion about the room. The setting was understood, and the attention of the room was not the problem.
The problem was not stage fright or not knowing how to present. The body would not allow the presentation to continue in the expected way.
That difference matters. A person can know what they are trying to say and still need a backup way to communicate when the body interrupts the explanation.
Gratitude
Thank you to the FNDS Society, the conference team, reviewers, organizers, volunteers, clinicians, researchers, advocates, and attendees who made space for this poster.
Baltimore brought real human connection through conversations with people living with FND, studying FND, treating FND, and advocating around FND. Those conversations are part of the project’s development.
Project Fionigan is not only about records. It is about people, access, communication, and helping important information follow the patient.
Step 1 — The abstract
The abstract is the official conference version. It explains the problem: FND was not understood early enough, records were scattered, communication failed, and the ER situation escalated.
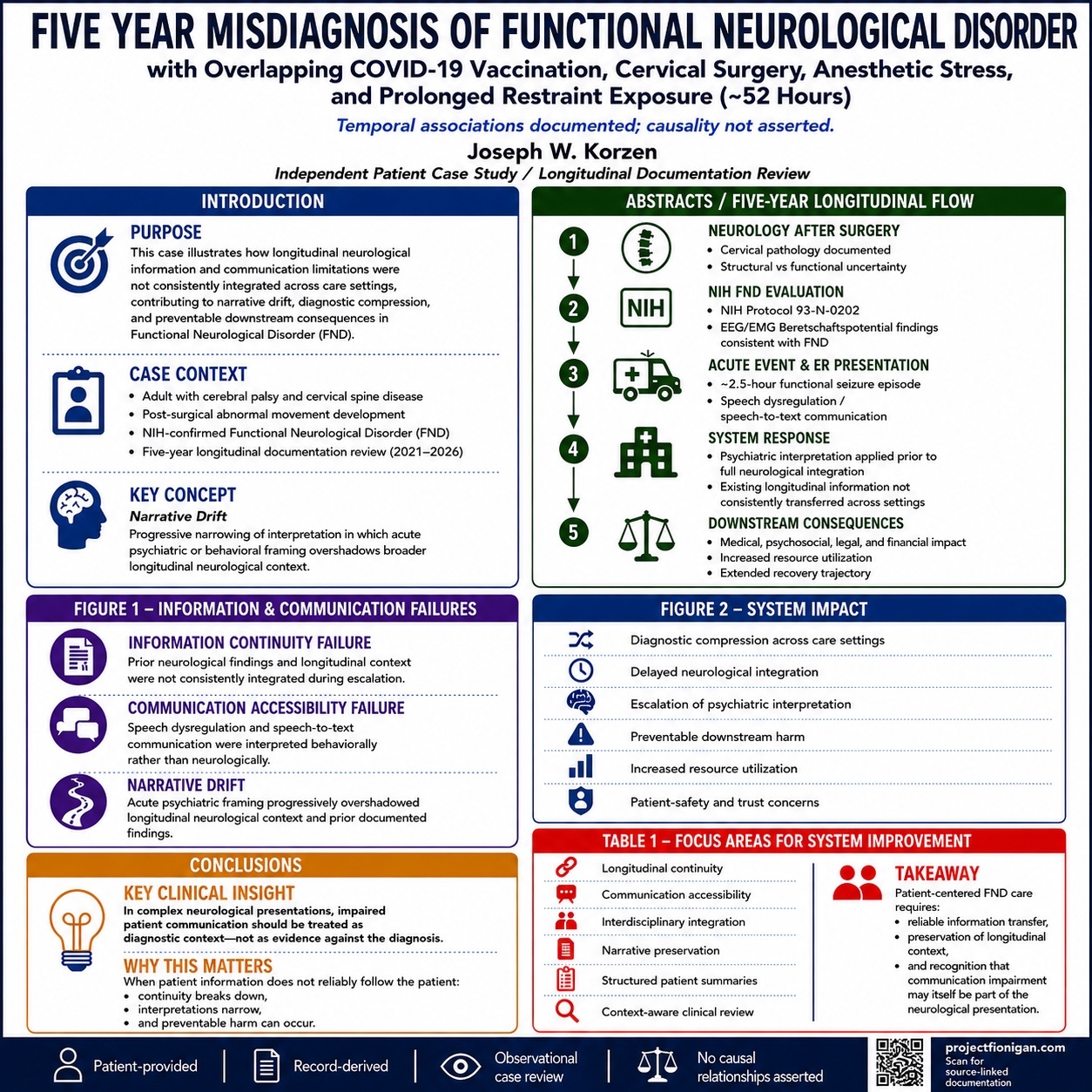
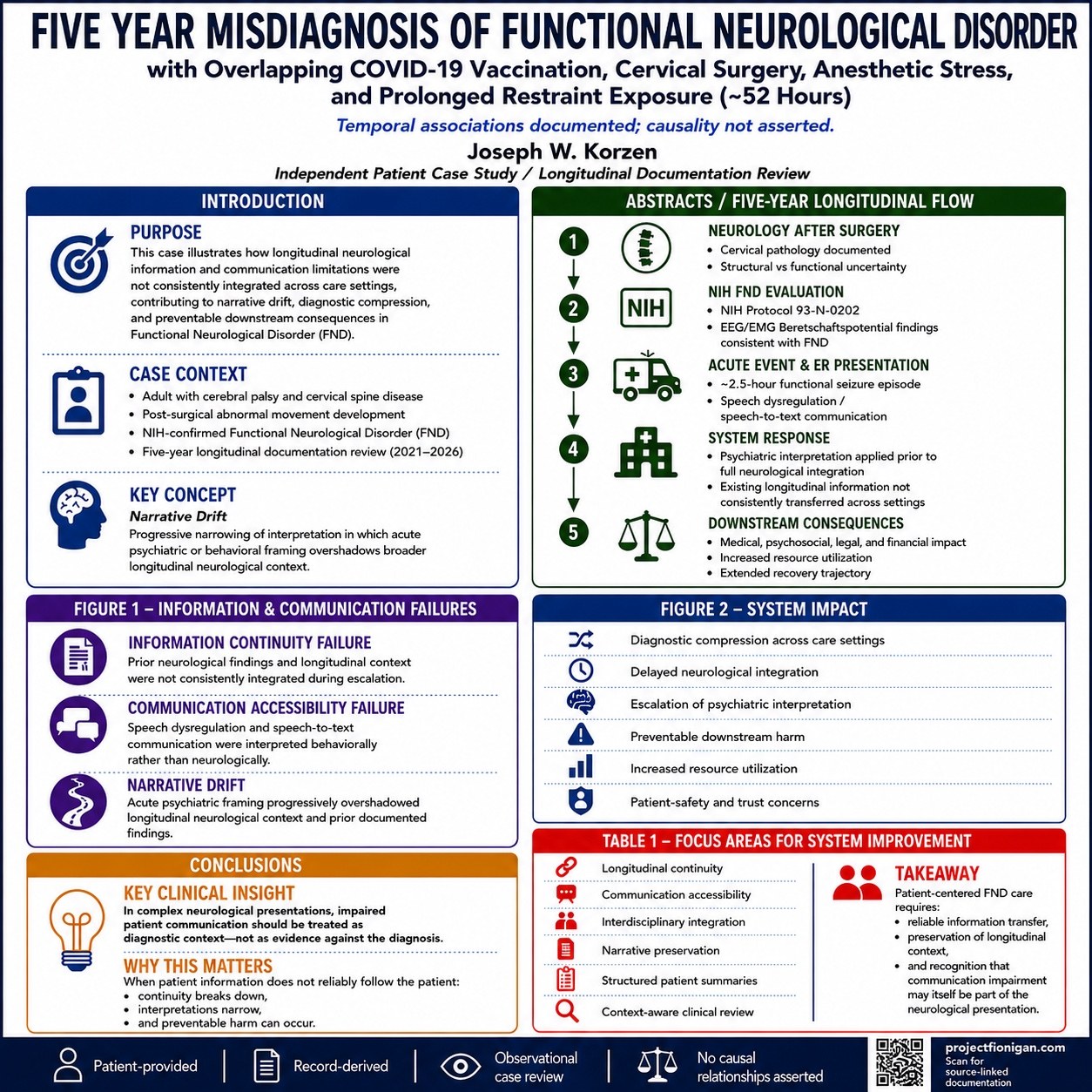
Functional neurological disorder (FND) is now defined as a rule-in diagnosis based on abnormal brain-network activity rather than structural lesions. Early identification is essential because premature antipsychotic medication and coercive restraint aggravate symptoms and generate legal consequences. FND diagnosis was verified by NIH-funded research protocol Diagnosis and Natural History Study of Patients With Neurological Conditions.
2021 - After a COVID-19 booster: progressive upper-body tightening with fatigue; CICP claim.
2022 Sept - cervical-spine ACDF: persistent foraminal stenosis. Intra-operative “fighter-flight” stress triggered functional symptoms.
2023 Oct - academic referral center EMG: chronic cervical radiculopathy, mild right median mononeuropathy; no brachial plexus injury. Pinched nerve at cervical post-op.
2023 Dec - NIH EEG/EMG: Bereitschaftspotential and no epileptiform activity; functional chorea confirmed.
2025 Feb - 2.5-hour non-epileptic seizure: ED diagnosed “psychotic break,” gave haloperidol 5 mg IM + risperidone 1 mg q12h before neurophysiology, issued TDO. Called 911 after staff refused release; handcuffed to bed 52 hrs, accused of “eloping.”
Text-to-speech request for GP ignored; returned without GP involvement. This is a local hospital that has all my data. I’ve been going there for years.
A patient-led review applied audit-style validation to create a five-year de-identified case file.
Systemic failures:
Onabotulinumtoxin A trial showed no benefit beyond CBT, confirming need for diagnostic confirmation before intervention. BMJ review stresses early rule-in diagnosis and rehab improves outcomes. Multiple triggers — vaccine, incomplete surgery, anesthetic stress — converged to produce FND; misdiagnosis snowballed into medical-legal crisis.
Vizcarra JA et al. Onabotulinumtoxin A and CBT in functional dystonia. Parkinsonism & Related Disorders.
Source: FNDS 2026 Conference Abstracts PDF. Additional references are listed in the abstract book after this entry, but the extracted snippet provided here cuts off immediately after the Vizcarra citation.
In plain language: Abstract 178 says delayed FND recognition, scattered records, communication failure, psychiatric framing, and ER/legal escalation all became part of the same crisis.
Official FNDS abstracts page: 2026 Conference Abstracts.
The abstract is reproduced as accepted for FNDS 2026 and reflects the author’s submitted recommendations. It is not a clinical practice guideline.
Project Fionigan does not diagnose, replace medical records, provide medical advice, or make clinical decisions. It is an all-inclusive accessibility-first continuity program that helps keep the story, records, questions, and communication needs together.
Poster image
How the project got here
Project Fionigan carries forward more than 30 years of experience with school-system technology and school-nutrition data. That work required accurate records, validation, deadlines, corrections, and audit trails.
When the medical journey required fragmented neurological records to be reconstructed, the same systems discipline revealed the central disconnect: the information existed, but it did not reliably follow the patient.
Project Fionigan applies that approach to FND and medical continuity. It takes unorganized medical records, dates, notes, test results, questions, corrections, and communication needs; keeps them connected to their sources; organizes them into a clear chronology; and makes the result human-readable.
The method does not depend on one provider, file type, or medical system. This website intentionally stays centered on FND, FNDS 2026, the poster, the handout, and the one-page medical continuity report.
Record-transfer lane
The records did not simply follow the patient. They had to be gathered, requested, packeted, transferred, and reassembled across many systems.
This is the same logic that came from decades of school nutrition, direct certification, eligibility, and audit work: the source trail has to match, and the handoff has to be verifiable.
Step 2 — The poster
the patient-author’s poster was part of FNDS 2026 in Baltimore. Abstract/poster listing: 178.
Step 3 — What happened in real time
The diagnosis, data, and communication attempts existed. The problem was that the information did not follow the patient clearly when decisions were being made.
During the Neurology track at this FNDS conference, the same pattern became visible again. The difference was more time, recognition, and self-regulation. After time spent learning the pattern, it became possible to stay with it, communicate around it, and keep it from taking over. The website became the backup when lived speech could not carry everything.
This conference also showed the difference between having FND around family and friends and having FND in public.
The symptoms were not new. The audience was new.
In private life, family and close friends may already understand parts of the pattern. In public settings—conferences, apartment viewings, clinical rooms, advocacy conversations, and professional spaces—the same symptoms can feel new, exposed, and harder to explain.
Project Fionigan exists for that transition point.
It provides context when a person cannot explain everything lived. It gives the record, communication need, symptom pattern, and next step a place to remain connected while the person learns how to navigate FND publicly, one day and one setting at a time.
Rehabilitation and continuity
Physical and occupational therapy helped me learn how to work with changes in movement, function, and communication.
How it works
The one-page report is part of an all-inclusive accessibility-first continuity program designed to help the most important information follow the patient when speech, typing, memory, stamina, or lived explanation becomes difficult.
It can organize the timeline, key sources, communication needs, corrections, and open questions into a short, human-reviewable format.
The working report and underlying medical records remain private while the all-inclusive accessibility-first continuity program continues to be reviewed and developed.
Case-study preview
In February 2025 a prolonged non‑epileptic seizure left the patient-author unable to speak clearly or operate a phone. Seeking care at a local hospital, he explained his existing diagnoses (childhood neurologic history and functional neurological disorder), requested his primary physician, and asked for a neurology consultation. Instead the case was reframed as a psychiatric emergency, he was transferred to a behavioral unit, and he spent more than prolongeds in restraints. Clinicians documented multiple psychiatric diagnoses even as notes described his thought process as linear and cooperative.
This case illustrates why continuity tools are needed: crucial facts (medical history, diagnoses, prior providers, communication needs) were not carried forward when decisions were being made. Without a bridge, the hospital staff saw only a distressed patient, not the established pattern of FND and previous evaluations. The resulting misclassification caused harm and delayed appropriate care.
Open the de-identified case-study page
Source-map note: Redacted supporting documents are available through the de-identified source-map page. Public text remains de-identified.
Public de-identified image
This image is public because it does not show the raw record packet, names, addresses, case numbers, provider names, or medical-record identifiers.

Boundary: identified court, hospital, lab, email, and source documents remain private. This image is presented as a de-identified visual anchor only.
Conference handout
What happened in the Neurology track looked like the same kind of escalation pattern from the ER, but this time the outcome was different.
This time there was more time, recognition, and self-regulation. The pattern could be managed, communication could continue around it, and it did not take over.
One-page report
The public one-page report structure is restored as de-identified framework content: the front page is history, and the back page is the continuity/action side.
Source map and technical closeout
The public site keeps the human story first. The de-identified source map, flat files, closeout entries, and technical source-status tools remain available here for readers who want to trace where information comes from.
One-page report
The public webpage now shows the actual back-page continuity printout. The front/photo/history side is download-only.
Post-closeout source-map additions
The latest records are represented as public-safe source-map entries only. Raw documents are not public.
Final source anchors
The closeout source map now includes de-identified anchors for unanswered FND-author outreach, FND Hope routing, the governor/kernel file, and the FND Society / FND-resource outreach placeholder.
Source map
The newest records are represented as source-map entries and plain-text de-identified summaries. Raw documents are not public.
Source map
The raw documents are not public, but the site now includes plain-text source-trace files showing where the information comes from.
Flat de-identified records
De-identified flat source files have been added for the orthopedic/spine chronology. These files are plain text and do not use the overlay.
Public de-identification
Patient-specific names, provider names, facility names, email addresses, record identifiers, exact identifying routes, and raw source records are removed or generalized in this public website version.
Objective source status
Open the source-status index to see what is already on the site, what is staged privately, and what still needs upload or redaction.
Official source bridge
The NINDS Functional Neurologic Disorder source is now available through a Project Fionigan landing page and source bridge.
Downloads
Coming soon
A moderated question-and-answer section is planned for questions about FND, Abstract 178, the poster, the one-page report, communication access, and Project Fionigan.
Questions and answers will be reviewed before publication and linked to objective sources where possible. Published answers will be informational and will not be medical advice.
Private medical information should not be submitted publicly. Supporting documentation is retained; documentation requests will be reviewed separately and remain patient-controlled.
Email a question or documentation requestContact
Use the conference app for networking, or click the email address below to contact the patient-author.
Please do not send private medical records through this public contact route.
Use these controls to listen, pause, resume, stop, or change speed. The Follow yellow button in the floating tray highlights the current word and follows the reading.
Default reading is Read all line by line. Read page order is the shorter normal page reading order.
The Play button uses Read all line by line by default.
Search a word or phrase on this page. Results jump to matching sections.